

By Susan BranscomeBoard member, recovered Food Addict Abstinence, in the context of Food Addiction, means choosing not to consume foods that trigger compulsive eating, cravings, and loss of control. For those struggling with addictive eating behaviors, abstinence is not about counting calories or following a diet plan; it is a commitment to remove substances that hijack the brain’s reward system. This approach creates the psychological and physiological space needed to heal, think clearly, and build sustainable and healthy patterns. To abstain from foods that trigger addictive physical responses or behaviors can free those who struggle with Food Addiction. What Is Addiction and Ultra-Processed Food? Addiction is a chronic brain disorder characterized by intense cravings, loss of control, and continued use despite negative consequences. Traditionally applied to substances such as alcohol or drugs, growing evidence suggests certain foods — especially ultra-processed foods (UPFs) — produce similar effects in some individuals. UPFs are industrially manufactured products high in sugar, refined carbohydrates, fat, and additives, engineered to be highly palatable and immediately rewarding to the brain. They may stimulate the same neural reward pathways implicated in substance use disorders, leading to compulsive eating, cravings, and physiological dependence. Neurobiological research shows that UPFs can trigger dopamine responses in reward centers of the brain, similar to addictive drugs. While the scientific community continues to debate how to classify this condition formally, many clinicians and researchers acknowledge that ultra-processed foods can cause addictive-like responses in a portion of the population. What Is Misunderstood About This Addiction and Using Abstinence? A major misunderstanding is equating recovery from addictive eating with dieting. Diets typically focus on restriction, weight control, and food rules — but they do not address the neurological and psychological grip that UPFs can exert. Recovery from Food Addiction is not about moderation or balanced eating alone; it’s about removing the trigger substances from an eating plan so that the brain can recalibrate. For an addict, even one bite of a trigger food can reignite intense cravings and loss of control, just as alcohol is unsafe for someone in recovery from alcoholism. Another misconception is that Food Addiction is purely a behavioral issue or a lack of willpower. In reality, addictive eating involves complex interactions among neurobiology, environment, stress, emotion, and habit. Abstinence is not punishment; it’s a protective practice that allows the nervous system to settle and the person to regain management and experience freedom from eating behaviors. Why It’s Not a Diet Food Addiction recovery differs from diets in fundamental ways: Ways to Recover Recovery from Food Addiction is most successful when abstinence is paired with supportive, evidence-based strategies that address behavior, cognition, and environment: 1. Cognitive Behavioral Therapy (CBT)CBT helps individuals identify the thoughts and patterns that lead to compulsive eating, and replace them with healthier coping skills. This is particularly valuable once trigger foods are removed, allowing greater clarity and self-regulation. 2. Peer Support & 12-Step ProgramsAbstinence-based groups such as 12-step fellowships provide community, accountability, and a structured path for ongoing recovery. 3. SMART RecoveryA secular, science-based alternative that uses tools from CBT and motivational psychology to manage urges, improve emotional regulation, and build self-empowerment. 4. Professional CounselingTherapists trained in addiction, trauma, and/or eating behaviors can help address underlying emotional drivers of Food Addiction. 5. Nutritional GuidanceWorking with nutritionists who understand addictive eating can help individuals identify trigger foods, stabilize blood sugar, and create personalized, sustainable eating patterns to reach a healthy body weight. 6. Lifestyle SupportsMindfulness, stress management, physical activity, and supportive relationships all reinforce the internal changes needed for long-term recovery. In Food Addiction recovery, abstinence is a state of mind and a way of living that frees a person from the chemical and psychological grip of addictive foods — not a transient diet trend. It represents a conscious commitment to protect brain health, emotional stability, and long-term well-being by removing substances that repeatedly cause harm. Rather than narrowing life, abstinence expands it — quieting obsessive food thoughts, restoring clarity, and allowing individuals to engage more fully with their relationships, work, and purpose. When the addictive stimulus is removed, the brain and body are given the opportunity to heal. Cravings lessen, mood stabilizes, and the constant internal negotiation around food begins to fade. From this foundation of stability, real recovery becomes possible — not just improved eating behaviors, but deeper emotional growth, improved physical health, and sustained freedom from relapse cycles. This path is grounded in science and strengthened by connection. Recovery thrives when abstinence is supported by evidence-based tools, compassionate professionals, and communities of people who understand the lived experience of Food Addiction. Together, these supports transform abstinence from an act of restriction into a pathway of empowerment, healing, and lasting change.
Can GLP-1s “fix” Food Addiction?
By Michael PragerChairman There are the causes of disordered eating. And there are the popular remedies for it. GLP-1s are the unprecedented, overwhelming favorites right now, hailed as life-changing by users who report significantly lower “food noise,” easier appetite control, and other benefits. But before them there was bariatric surgery, and before that a legion of diets, fad and otherwise. All these techniques have helped some people reduce their body weight, with varying levels of side effects and long-term success. But a question rarely asked is, how did these patients reach the metrics that qualified them for Ozempic (and the like), or for the various bariatric techniques? GLP-1s mimic the natural GLP-1 hormone to slow gastric emptying, increase satiety, reduce appetite in the brain, and stimulate insulin release. Bariatric procedures reduce stomach size while affecting gut-brain signaling in ways that promote earlier satiety, lower appetite, etc. But did patients lack natural GLP-1, or did bariatric patients have stomachs that were too big? Or do the techniques address unwanted outcomes of different origins? GLP-1 medication, bariatric surgery, and OG diets have helped people to lose weight — and sure, that’s why people have turned to them. But none of them get at the “why,” as in, “what factors led to my needing drugs, surgery, and/or diets?” We’re not talking about fault. Addiction is a brain disease that causes some people, based on their physiology, to react differently to substances and/or behaviors than other people do. People with or without this physiology can be driven to overeat by unresolved trauma and many other causes. Our experience with Food Addiction tells us that these factors are very often more important to address than how or how much one eats. That’s why Food Addiction is not defined only, or even chiefly, as a weight issue. And that’s why techniques to lose weight can improve one’s health prospects. But without facing the fullness of one’s situation, even the best weight-loss solutions are unable to bring the serenity that results from identifying and working to ease what underlies one’s behaviors.

GLP-1 explainer discussion
The National Academy of Medicine summarizes a conversation among specialists from two universities, the Cato Institute, and the Obesity Action Coalition about the current state of GLP-1s. Here are some of the subject headings, if you’d like to read more: Obesity Is a Complex Chronic Disease and Still Highly StigmatizedGLP-1s Are SafeGLP-1s Are Expensive, But Changes Are ComingAre GLP-1s Worth the Cost? ProbablyJust Increasing Access to GLP-1s Is Not Enough The academy describes itself as offering independent and evidence-based. guidance on healthcare policy decisions. It has operated since 1970.

Children and the new dietary guidelines
Children and the new dietary guidelines By Cynthia Myers-Morrison EdDBoard member Nearly everyone has heard some kind of commentary about new dietary guidelines issued Jan. 7 by the US government. So, what are the changes and how do they impact children and families? The guidelines suggest prioritizing protein, dairy, vegetables, fruits, healthy fats, and whole grains. Suggestions include non-supersized portions and limiting added sugars, sodium, and highly processed foods. Perhaps the most challenging thing for everyone involved is the identification of NO ADDED SUGAR for children under 11 years of age. Even fruit juices, if consumed at all, should be watered down considerably. So, how do we adjust to these guidelines, to make the transitions as seamless as possible? Motivation Sometimes the big WHY is helpful. The government document, issued jointly by the departments of Health and Human Services and Agriculture, provided the following statistics: According to a recent analysis by Johns Hopkins, 48% of all federal tax dollars are spent on health care – and 90% of U.S. health care spending is on people with chronic diseases. Many of these conditions are preventable, often reversible, and often tied to the food we eat. The United States faces the highest obesity and Type 2 Diabetes rates (OECD) in the developed world. “The United States spend 2.5 times more per capita than the average of developed countries (OECD) on health care – and our life expectancy is 4 years lower. Chronic conditions tied to food are major contributors to this. “The US childhood obesity rate is nearly five times higher than other developed countries. “In the United States, one-third of teens are prediabetic, a fifth of children and adolescents have obesity, and almost as many young adults have nonalcoholic fatty liver disease. “ 77% of military-aged youth aren’t eligible to join the military – primarily due to chronic diseases tied to food. “A recent study of Medicare beneficiaries found that a 15% weight reduction resulted in nearly $1,000 per year in lower Medicare spending.” Yet another benefit It could be said that more money would be available to spend on programs for school-aged children and adolescents, if these issues were addressed. Your informed dietary choices shared in your family and community can make the difference for your children and family and then ripple out to your friends’ families and entire communities. Parents may want to talk with their pediatricians about their infants and toddlers after reading the guidelines. For about the first 6 months of life, only breast milk is recommended. When it is not available, iron-fortified infant formula is suggested. Continuing to breastfeed for 2 years or for as long as it may be mutually desired by mother and child is recommended. More specifics are shared, especially about potential allergy inducing items and what to do. Here’s some more information adapted from the new guidelines: Infancy and Early Childhood (Birth to 4 years)

Gudmundsdottir stepping down
Gudmundsdottir stepping down from INFACT leadership Esther Helga Gudmundsdottir of Iceland is stepping down from leadership of the INFACT School.. “I have research and writing obligations to fulfill. Once I let go of working in treatment and the INFACT School, I hope to have the energy to get it all on paper,” Gudmundsdottir said. Gudmundsdottir, a past chairwoman of the Food Addiction Institute, founded the school a decade ago, and began awarding certifications in 2017. More than 130 students from almost 20 countries are now certified Food Addiction professionals as a result. Esther was an early participant in the ACORN Professional Training Program, which was operated by Phil Werdell, the institute’s founder. A substantial step forward from her own training was that, for INFACT, she affiliated with the European Certification Board, adding institutional endorsement to her students’ diplomas. “Esther Helga has worked tirelessly educating the public in Iceland and throughout the world about Food Addiction and its treatment, and her contributions to the field cannot be ignored,” said Mary Foushi, ACORN co-founder. “Her legacy will live on through INFACT, the professionals it has trained, and the Food Addicts who’ve been led to recovery.” Gudmundsdottir announced her decision to the INFACT community last month, expressing the hope that new leadership will emerge. In an interview, she said, “What I hope is that people will step up to continue our mission.” Esther Helga Gudmundsdottir Gudmundsdottir, a recovering Food Addict herself dedicated to abstinence from binge and trigger foods and behaviors for late-stage Food Addicts, has operated MFM, a treatment center in Iceland that has treated more than 3,000 Food Addicts, since 2006. In 2014, she organized a conference on Food Addiction in Reykjavik. At the end, participants formed Matarheill, an organization of health professionals advocating for Food Addiction’s inclusion in Iceland’s national healthcare system.

Carlos Zumarraga
Edit Template Clinica Keto Merida, Yucatan, Mexico Email Telephone On the Web “Sugar Sober” Dr. Zumarraga is an MD/Scholar. He founded Clinica Keto and is the author of “Sugar Sober.”
Brian Baumal
Edit Template Aliva Psychotherapy Toronto, Canada Email Telephone Website We assess every patient that uses our services into three large groups: 1) Weight management, 2) Eating disorders 3) Food Addiction. We provide the relevant treatment based on the assessment. For Food Addiction and/or people exhibiting eating disorders AND Food Addiction, we use an abstinence-based approach, where we “sanely, intelligently, and compassionately” (so as to avoid “diet trauma”), remove suspected trigger foods. We monitor to ensure: 1) Instances of acute large eating episodes are reduced; 2) Food noise/cravings slowly go down to a manageable level over time.
An explosion of research
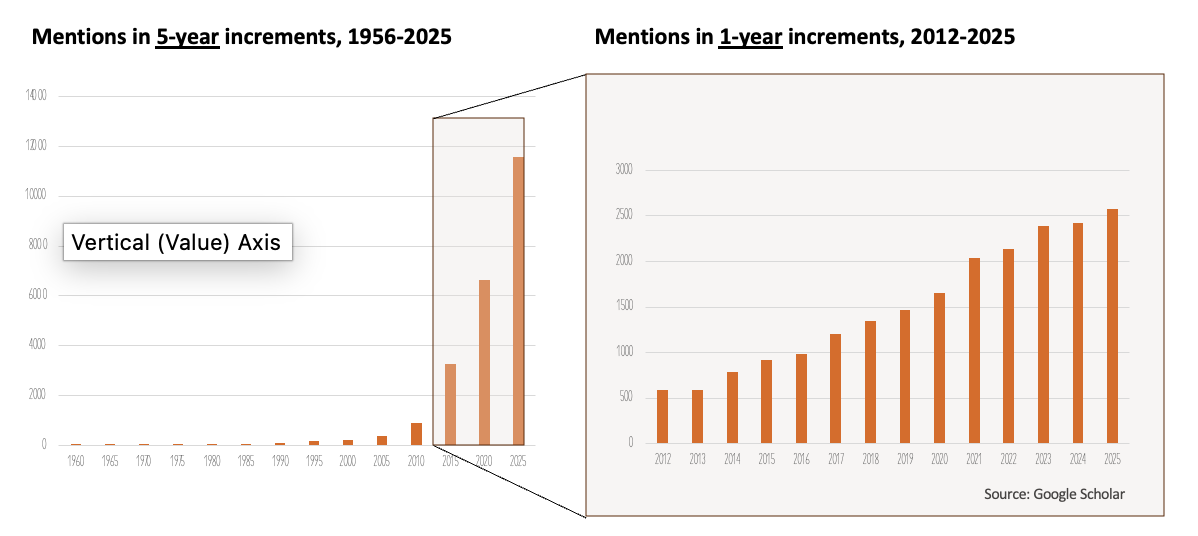
The institute has been working toward recognition for Food Addiction in the two key diagnostic manuals practically since it was formed in 2005. We could and did say what we knew about Food Addiction, but one of the rejoinders was, “where’s the research?” From when Theron G. Randolph introduced “Food Addiction” into academic literature in 1956, until the institute’s founding, fewer than a thousand studies mentioned the term. This is according to Google Scholar, which focuses on journal articles, theses, technical reports, etc., but leaves out news, editorials, and books. What about now? From 1956 through the end of last year, a Google Scholar query for “Food Addiction” returns close to 23,500, about 9 in 10 of those since 2012. A huge factor in that explosion is the Yale Food Addiction Scale, which was published in 2009 and made it much easier to screen for Food Addiction. It mirrors the American Psychiatric Association’s criteria for substance-use disorders and has been cited academically more than 800 times, according to the University of Michigan. It wasn’t until 2017 that more than 1,000 were published in one year, and last year, that number grew to almost 2,600. That’s 7 studies per day! Google Scholar is a blunt instrument for measuring this, but the numbers certainly show that researchers are well beyond the days when no researcher with ambition was willing to put “food” and “addiction” even in the same sentence. No one can ask anymore, “where’s the research?”

Q&A with neuroscientist Alex DiFeliceantonio
DiFeliceantonio, an appetitive neuroscientist at Virginia Tech, answers questions for Scientific American. Some excerpts: SA: What does it mean to have a “food addiction”? DiFeliceantonio: “When we’re thinking about food addiction and looking qualitatively at what people are eating when they are saying that they can’t stop eating, we have to put it in the framework of a substance use disorder. These disorders affect life in an untenable way. Food addiction isn’t in the Diagnostic and Statistical Manual of Mental Disorders (DSM) like substance use disorder is, but there is a proposal to have it put in the DSM. “We typically look to the Yale Food Addiction Scale for clinical evaluation. … If we accept that food addiction exists—if you give the Yale Food Addiction Scale to large population-level studies and do it across multiple countries internationally—we generally find that around 12 percent of people [experience] it. A combination of factors can lead to an addictive behavior. And the most common is the addictive potential of the substance combined with the vulnerability of the person. We think about both of those things with food, too: ingredients that could have addictive potential and the people who could be most vulnerable. …” SA: Why does “food addiction” ignite debate? DiFeliceantonio: “One pushback I hear is we don’t want to overpathologize everything. But I think that if about 12 percent of a population is telling you that they have a problem, maybe we should look at it, or we should at least give it some concerted study and determine what it is. People also say it’s a behavioral addiction — you are not addicted to food as a substance; you are addicted to the act of eating. But that argument falls down pretty quickly when you look at what people are eating. If you were addicted to the act of consuming, you would be eating things that were hard or crunchy or that required a lot of work to consume. And that’s not really what we see. We see people losing control over intake for items that are high in fat and sugar — refined carbohydrates. “I also think a lot of the pushback is a moral tie — if you’re addicted to food, you’re a bad person. For the most part, a lot of people have let this go. We understand that alcohol use disorder, for instance, isn’t caused by a failing of willpower. [People with the disorder] cannot overcome it, and we have to help them. I’m always bringing that level of compassion to food addiction, too.” SA: If ultraprocessed foods are truly “addictive,” what are some treatments? How should those treatments be tackled on a societal and individual level? DiFeliceantonio: “When someone has a substance use disorder, part of the treatment is for them to avoid the cues and context in which they use that substance. … Addiction is societal and behavioral. We decide what drugs are illegal. We decide at what age people have access to potentially addictive substances. Artificial refinements of foods — so pure sugar, fat, combinations of fat and sugar that don’t occur in nature—also activate our reward system. At what level is a rewarding substance one that we are willing to regulate as a society? … You need to eat to survive, but you don’t need the majority of ultraprocessed foods for human survival, food security and national security.”

Parent and child go hand in hand
By Cynthia Myers-Morrison EdDBoard Secretary The metabolic health of children and families is crucial to progress in addressing Food Addiction. Getting Ultra Processed Food Addiction as a substance use disorder into the DSM, the diagnostic manual of the American Psychiatric Association, is also essential because that will give adults access to treatment. These adults can then model healthier behaviors of abstinence from their trigger foods/substances and behaviors. With fewer foggy brains in households, workplaces, and society, better choices will be available. The next frontier: Revolutionize what we provide as food to children and families. Make it REAL FOOD. Many parents, grandparents, and other relatives in recovery have said, “Wait! I don’t want to limit my children’s access to the things I enjoyed as a child.” How many have said, “I don’t want to cause mine to be anorectic or a binge eater by limiting the choices they have for food items when other children have those items”? Does any child need sugar to survive? (Spoiler alert: the answer is a resounding NO!) Alternatively, how many have seen the Mike Collins YouTube episode about his children’s fetal development and the first six years of their lives with no sugar and limited carbohydrates? Their intellectual, physical, and relational development flourished while unimpaired by sugar. Mike came to understand that his mother’s description of him as her Little Angel was in fact his own sweat on the pillow in the form of a halo. He saw his own sons’ halos only at 6 years of age with their first consumption of sugar and the formation of their sweaty halos on their pillows as their young bodies sweated out the sugar. Alternatively, have you seen Agnes Bora describe her own food recovery and desire to change what her teens were eating? Use of alternative sweeteners in vegetables increased the consumption of them for her children. They’ve continued eating vegetables over their lifetimes and have passed on to their children the delight of eating vegetables. Sweeteners may not be a perfect solution; however, many agree with incremental improvements. Do we have to make the process of changing from the huge sugar consumption that we have now to no sugar consumption a stark black and white? Is it possible to make the changes more gradually with the alternative sweeteners? Harm reduction anyone? Listening to Andrea Tarka White speak about the challenges of her child and his sugar consumption and what she did to markedly change what he was eating may offer hope. Even in the face of doctors who were opposed to changes in her child’s eating, she persisted. Listen to her story and the outcomes. If parents can change their consumption patterns, why wait for another generation of impairment before the children change? Let us support them with the knowledge and goal setting of health, well-being, active lifestyles, and mental clarity to grow into metabolically healthy adults. REAL FOOD for Healthy Families. Your choice. (After all, who buys the real food or the sugary sweetened beverages?) Adults in the household can make new choices today with whatever clarity you are willing to share. Happy New Year.